Вход
Вход Регистрация
Регистрация





Миниатюры

Сообщение изменено: koelner (11 June 2008 - 11:12)


 27 голосов
27 голосов

Old School




Новичок

PioneerРон, типа, тоже не в форме, но о такой "неформе" не то что любители типа меня, да и соревнующиеся спортсмены наверно помечтать только могут
Новичок

сначала зашел на страничку Вишневского, посмотрел на его "никакую" форму и подумал - дай бог мне такую когда-нибудь..
а потом зашел сюда и понял, как все-таки их проффи далекоооо от наших... Рон, типа, тоже не в форме, но о такой "неформе" не то что любители типа меня, да и соревнующиеся спортсмены наверно помечтать только могут..
.
Differential diagnosis:
- 1) Cervical Spine Degeneration and Foraminal Stenosis. Because of the patient's age and history of heavy weightlifting
the most likely diagnosis here is degeneration of his cervical spine. This may be a result of degenerative bulging or
herniated intervertebral disks or facet hypertrophy with bony spurring causing compression of the exiting nerve root at the
level of the C7 nerve root. This could result in latissimus and triceps atrophy.
- 2) Partial Latissimus Tendon tear: Although his tendon feels intact and he does have a functional lat, he may still have
a partial tear of the tendon. Mr. Coleman has high pain tolerance and is quite stoic; thus his pain may not have been
elicited on physical exam.
- 3) Peripheral Thoracodorsal Nerve Impingement: This diagnosis is less likely, especially if the triceps atrophy and
weakness is a real issue. This could be a result of muscular impingement or a mass effect. If he ever had any site
injections in the region of this nerve there may be a sterile abscess. No lipomatous masses appreciated on palpation.
- 4) Thoracodorsal Nerve Injury: This would be possible with a misplaced site injection.
- 5) Left shoulder and elbow arthritis, bursitis, tendinitis: less likely diagnoses without any loss of range of motion,
crepitus, or pain to palpation/with motion
- 6) Cancer, systemic illnesses, and myositis: Even less likely with lack of consistent history and constitutional
symptoms. [When you hear hoofbeats in Texas, don't look for Zebras.]
Family History: Noncontributory.
Social History: Retired police officer and professional bodybuilder, denies tobacco use, occasionally drinks alcohol, and
denies recreational drugs and anabolic steroid use.
Review of Systems: Patient denies any other constitutional complaints, bowel, bladder, liver, endocrine, neurological,
musculoskeletal, renal, pulmonary, or skin complaint at this time.
Focused Physical Exam:
General: Patient is a 42y/o, 5'11", 315lb massive bodybuilder in no acute distress. He's alert and oriented. Patient
appears his stated age.
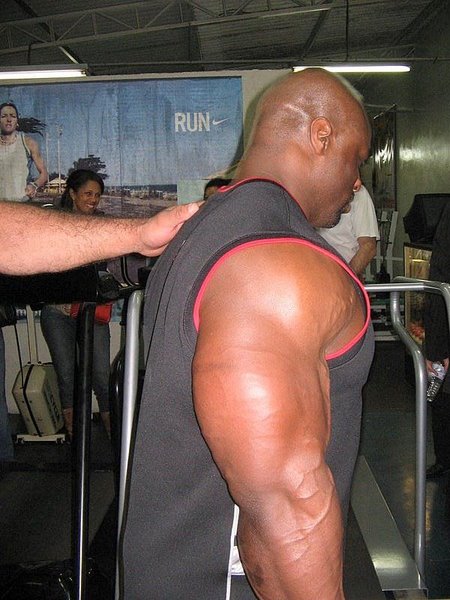
Left upper extremity:
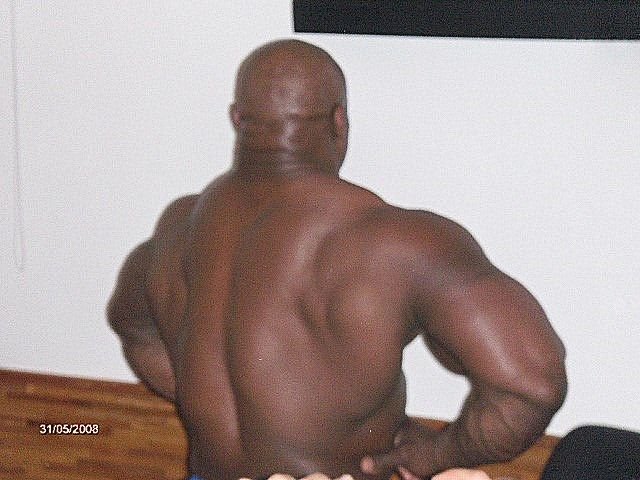
Inspection and palpation: Noticeable atrophy of the left latissimus dosi muscle in comparison to the right. Mild left triceps
atrophy compared to the right. No palpable masses around left shoulder. No tenderness to palpation of cervical spine,trapezius or latissimus. No palpable muscle defects. Tendons appear intact. Skin is intact without rashes, erythema or
fluctuance. Compartments are soft.
Range of motion: Full to shoulder forward flexion and abduction, elbow flexion and extention, forearm supination and
pronation, wrist flexion and extension and digital motion. No crepitus or pain with passive or active motion of those joints.
Full cervical spine range of motion, with mild pain in left arm with neck extension.
Motor: 5/5 strength to shoulder abduction, elbow flexion, wrist extension, hand intrinsics, EPL and FPL. 4/5 strength to
shoulder extension, elbow extension, and wrist flexion.
Neurologic: Light touch sensation C5,6,8 and T1 intact. Diminished subjective sensation in the C7 dermatome; middle
finger. No long-tract signs-clonus, hoffmans, babinski (no spinal stenosis), globally diminished reflexes (often hard to get
bodybuilders to relax). Negative Roos Test (no thoracic outlet syndrome). Normal rectal tone per the eager intern.
Vascular: 2+ radial pulses equal bilaterally with regular rate, brisk refill in all digits
Мозг Форума
Без согласия пациента такая информация не разглашается!Мне непонятно только, как в Америке обстаят дела с врачебной тайной? И насколько допускаются опубликование подобных вещей?
Новичок

Новичок
Новичок
 .Связки у суставы у них очень крепкие .а вот мышцы не выдерживают нагрузок
.Связки у суставы у них очень крепкие .а вот мышцы не выдерживают нагрузок
Сообщение изменено: провизор (17 June 2008 - 06:04)
Новичок

Мне тоже так кажется.)) Ток не суставы рвутся, а связки (соединительная ткань).вязки у суставы рвутся а не сама мышца так как мышца выдерживает а вот всё остальное нет

 Наверх
Наверх