Вход
Вход Регистрация
Регистрация





C Новым 2021 годом!!!
Здоровья всем!!!


 29 голосов
29 голосов

человек

Саша уже отметил?))),( Отмечаешь?))
Бокал выпил под бой курантов, проводил високосную Крысу.
Этот раз мы вдвоем с женой...))) Вся остальная семья по своим компаниям разбежалась.
Хотя... Вру... Еще с нами три кота...)))
жирный монстр-эстет , грузчик)колхозник)больной старик))
Романтично)Бокал выпил под бой курантов, проводил високосную Крысу.
Этот раз мы вдвоем с женой...))) Вся остальная семья по своим компаниям разбежалась.
Хотя... Вру... Еще с нами три кота...)))
Сообщение изменено: Горец67 (01 January 2021 - 12:55)
жирный монстр-эстет , грузчик)колхозник)больной старик))
поздравляю с Новым годом!Каждой твари - по паре, а каждой паре - по Талавари!
человек
Как противнику спорта, любителю сигар и выпивки Черчиллю удалось прожить 90 лет

Интересующийся

Если не ошибаюсь, про Черчилля писали, что у него в 44 года поставили онкологический диагноз (был ли такой в то время?), и он с ним прожил еще почти полвека - ему и без Терафлю было некогда болеть!
Сообщение изменено: калыван (23 January 2021 - 05:22)
Интересующийся
55кг на 90 повторений. Свой вес 86,5 - коэффициент 57,225. Действующий рекорд Мира НАП в этом весе и возрасте - 56,222 (МСМК НАП в этом весе - 71 повтор)
Сообщение изменено: калыван (29 January 2021 - 07:43)
Интересующийся
Да, похоже, тренер тут и не при чем: видимо, природные задатки + заниженный болевой порог. Я вот уже полгода топчусь на 51 повторе, оправдывая себя второй работой, недосыпом и т.д.Вадим, молодец и ученик и тренер!
Бывалый

и тренер!
Вначале немного "тормознул" 1мин 45 сек.
Ненужный вопрос ученика: "Сколько!!??". Лишняя энергия тратится.
Говорил бы каждый 5 или 10-й раз после 30-40 начальных.
человек
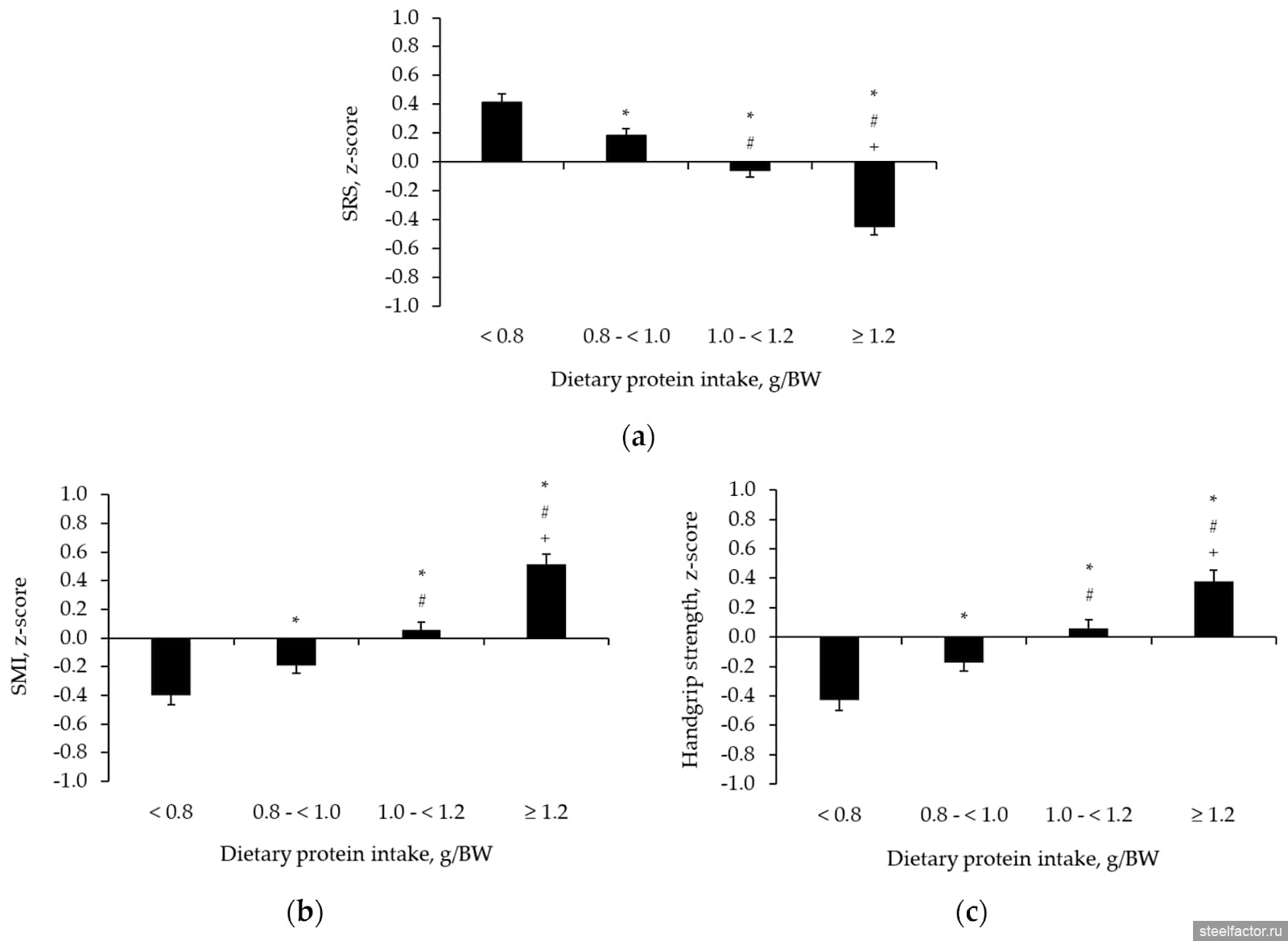
ПРОТЕИН У ПОЖИЛЫХ
Бывалый

Вот бли опасно! Сколько таких видео по ютюбу.Штанга на шею и не поднять
Может на видео не видно, у меня внизу есть рэк(страховочные стойки), поэтому никакого риска нет, не пожмёшь, опустишь на рэк и вылезешь из под него. Посмотри, с левой стороны видно одну блестящую стойку.
Сообщение изменено: montgomeri (06 February 2021 - 12:26)
Гедонист - экстремал

Может на видео не видно, у меня внизу есть рэк(страховочные стойки), поэтому никакого риска нет, не пожмёшь, опустишь на рэк и вылезешь из под него. Посмотри, с левой стороны видно одну блестящую стойку.
Да все там видно)
жирный монстр-эстет , грузчик)колхозник)больной старик))
человек
Немного "пищи для мозга". На мой взгляд материал интересный. Интересный именно тем что это ситуация из жизни. Кроме того тут есть и возрастная составляющая, и наличие в анамнезе анаболических препаратов (тема довольно много обсуждаемая):
,
Итак, джентельмен 54 лет, культурист (бодибилдер), который принимает фарм препараты.
,
Пациент обратился в отделение неотложной помощи с эпизодом острой боли в груди, сопровождающийся тошнотной, которая началась после интенсивной силовой тренировки. Боль усилилась в момент принятия душа. Через 3 часа он поступил в отделение неотложной помощи.
Вес 110 кг, ИМТ 37.
,
На основании клинической картины и данных ЭКГ диагностирован Инфаркт миокарда.
,
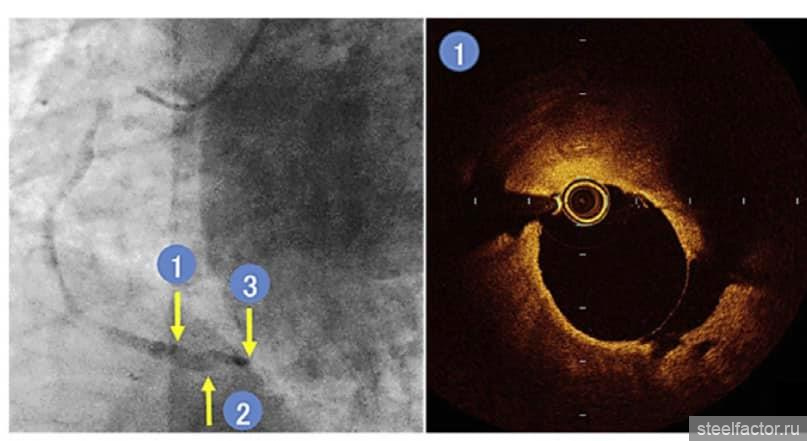
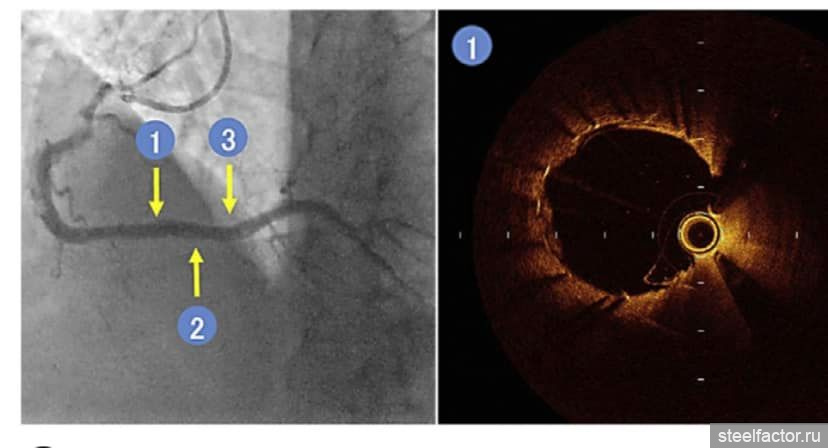
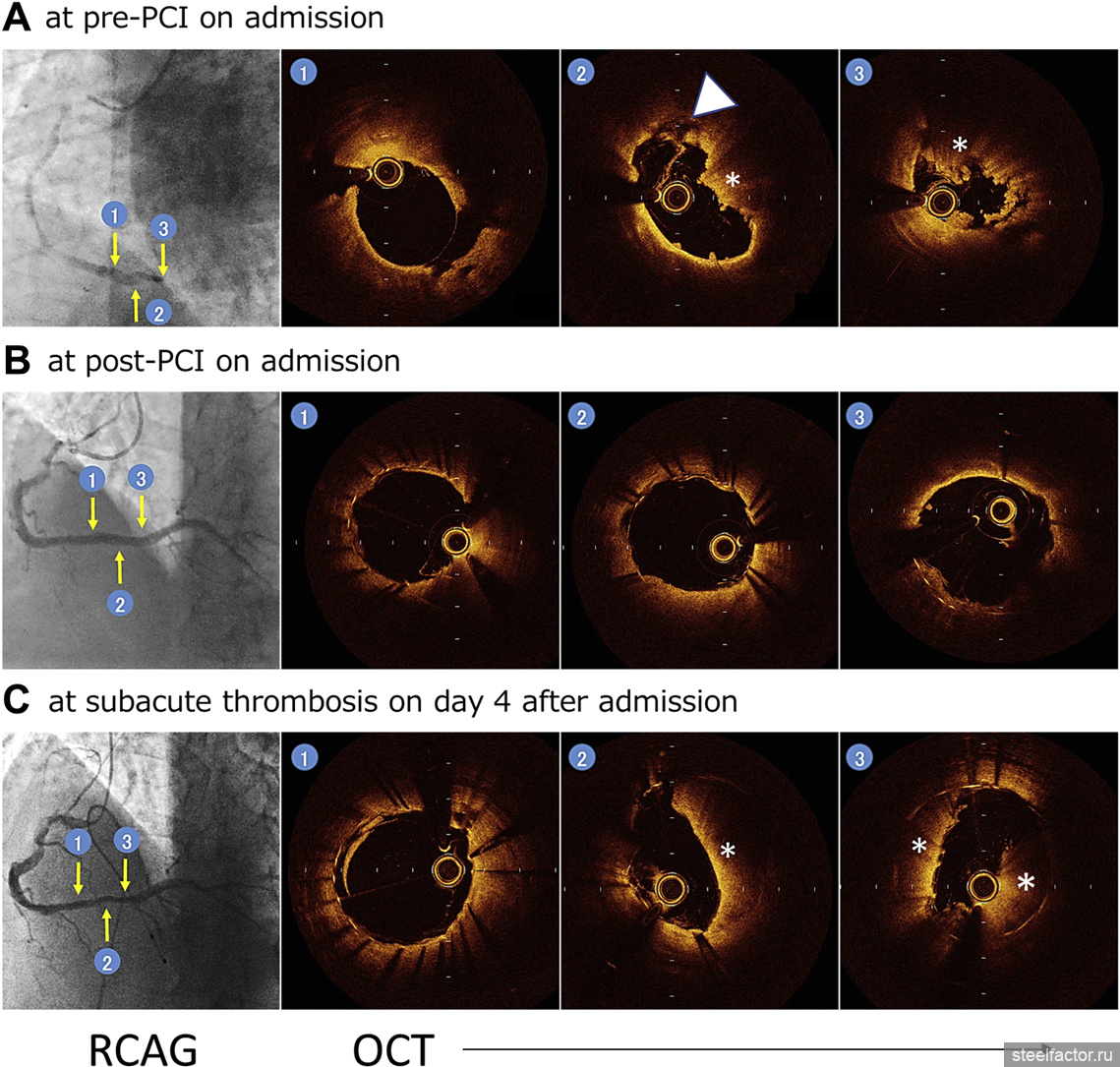
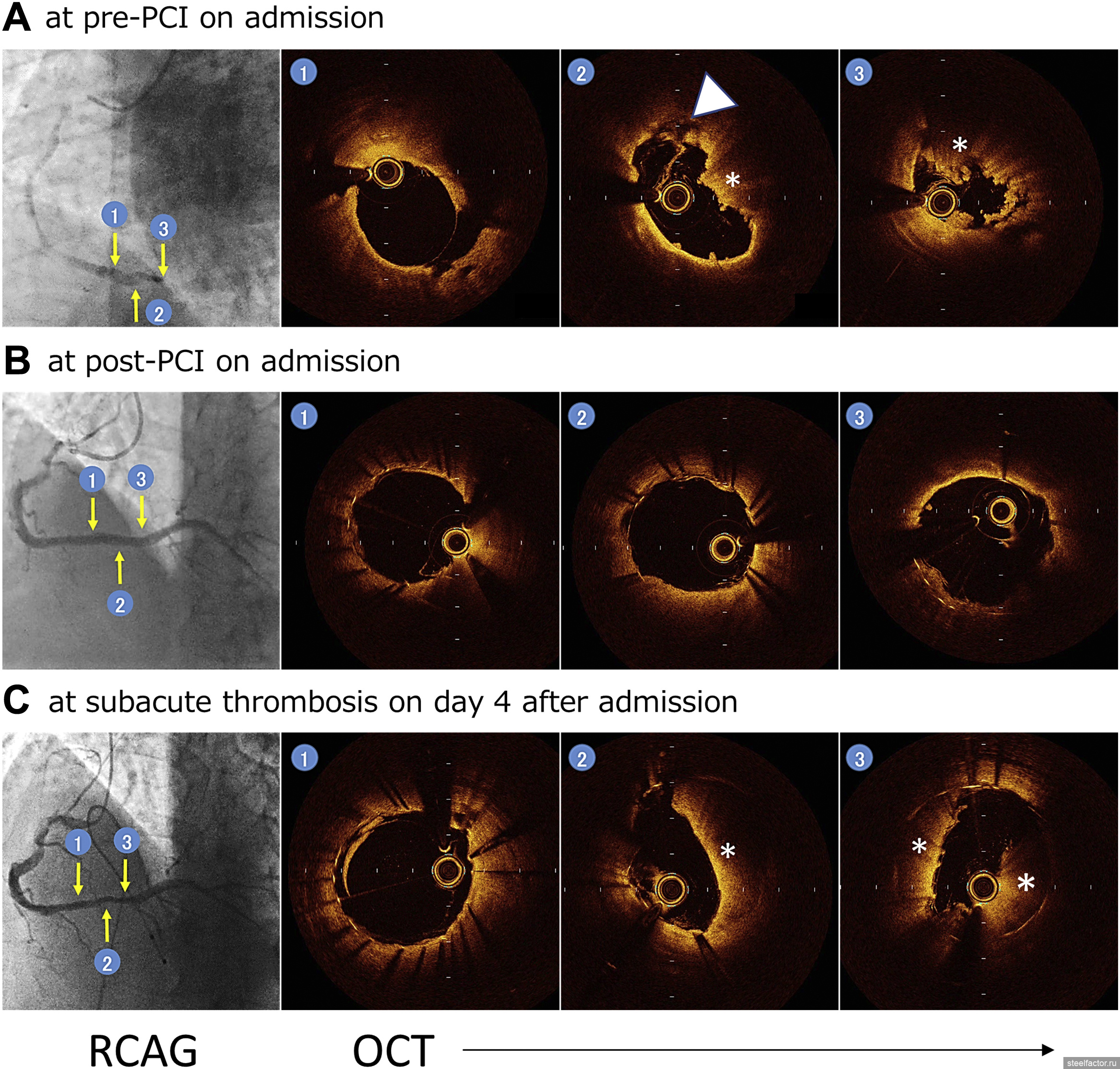
Пациенту было выполнена коронарография (КАГ), где было выявлена тромботическая окклюзия в дистальном сегменте ПКА (правой коронарной артерии). На ОКТ (оптическая когерентная томография) визуализировался разрыв атеросклеротической бляшки и образование тромба (рис.1)
,
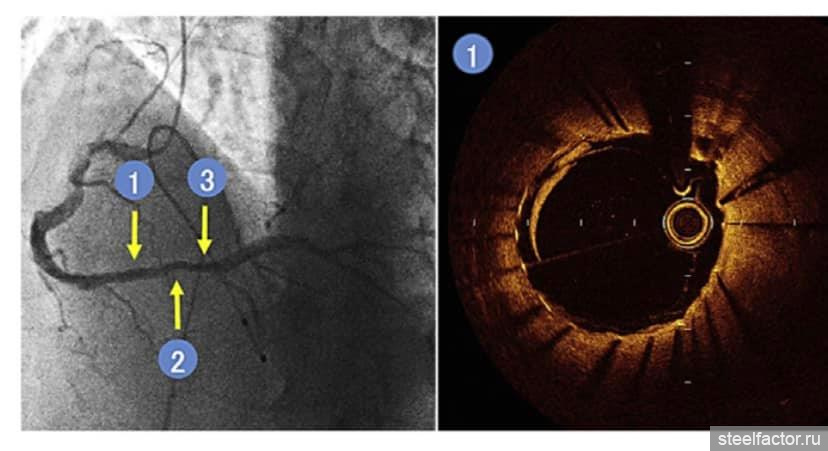
Пациенту выполнили экстренную ЧКВ (чрескожное коронарное вмешательство) с имплантация эверолимус покрытого стента в д/3 ПКА. На контрольной ангиографии хороший результат, диссекции по краям стента не выявлено, антенрадный кровоток восстановлен. На ОКТ подтвердился оптимальный результат стентирования. (Рис. 2)
,
На 4 сутки после поступления снова пожаловался на боль в груди. Нестабильная гемодинамика (гипотония, брадикардия). На ЭКГ элевация сегмента ST в нижних отведениях с полной АВ блокадой (типичная ситуация про окклюзии ПКА). На ЭХОКГ: признаки спортивного сердца (концентрическая гипертрофия ЛЖ с максимальной толщиной стенки 14 мм.
,
И тут выяснилось, что пациент изначально не сообщил, что в не медицинских целях в течении 2х месяцев принимал андрогены и анаболических стероидов: перорально оксандролон 20 мг, метандиенона 40 мг.
,
Пациент готовился к соревнованиям по бодибилдингу и в течении последних 3х лет циклически принимал анаболические стероиды и андрогены по схеме 3:1 (приём 3 месяца и 1 месяц отдых). (Рис. 3).
,
Пациент экстренно взят в рентгенооперационную с последующим выполнением КАГ и ОКТ, где был выявлен неокклюзирующий остаточный тромб в месте имплантации стента. Ангиопластика со стентированием не потребовалась. (Рис. 4).
,
Авторы исследования предположили, что тромботические явления могут быть частично вызваны некорректным употреблением анаболических стероидов.
,
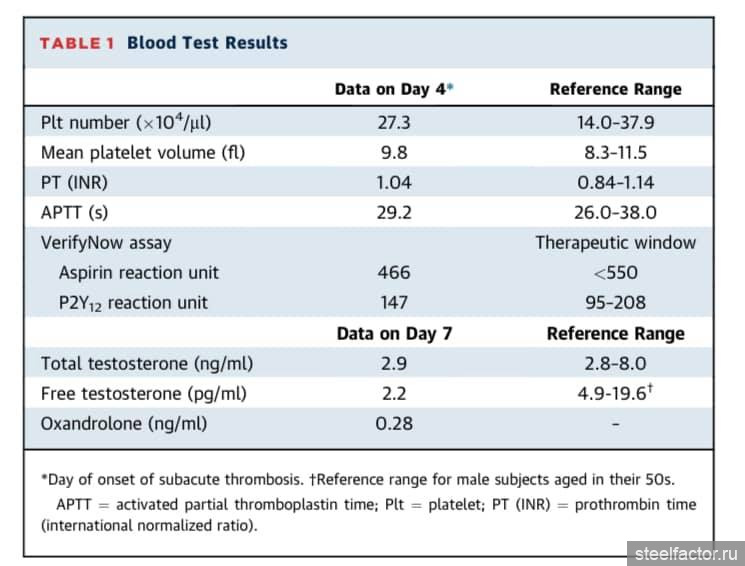
Причем концентрации тестостерона (общего и свободного) в сыворотки крови были низкие, однако у пациента не было клинических симптомов, связанных с гипогонадизмом.
,
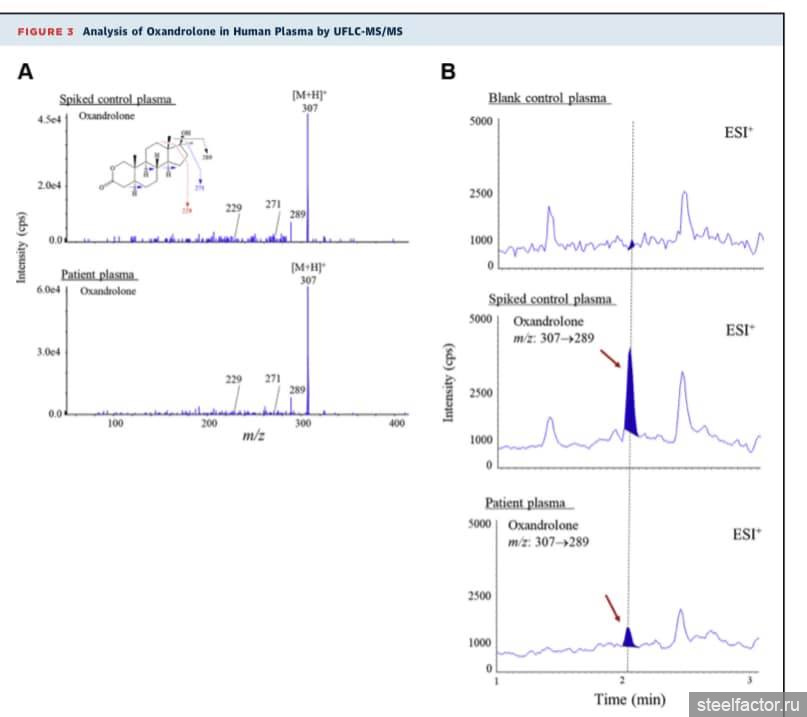
Также была проведена сверхбыстрая жидкостная тандемная хроматографическая массспектрометрия для обнаружения оксандролона и метандиенона в крови. В плазме было обнаружено только присутствие только оксандролонового соединения. Количественный анализ показал концентрацию оксандролона 0.28 нг/мл. Учитывая что метандиенон быстро метаболизируется, его соединение не нашли. (Рис. 5).
,
И так, подострый тромбоз стента развился несмотря на оптимальную двойную антиагрегантную терапию (аспирин + блокатор АДФ-рецептора).
Также у пациента была выявлена дисфункция печени. Поэтому дополнительно был назначен пероральный антикоагулянт прямого действия - апиксабан 10 мг/сут.
,
И так, коллеги, будьте острожны кто прописывает курс фарм препаратов болибилдерам. Сейчас это очень стало модно, причём онлайн. Такие спортсмены - пациенты в идеале должен быть обследованы. И весь курс андрогенами и анаболическими стероидами должен контролироваться специалистом (опять же в идеале если спортивный врач имеет ещё и лицензию диетолога, эндокринолога), либо несколькими специалистами.
И таких клинических случаев очень много.
,
Ссылка на статью:
,
==============
Subacute Stent Thrombosis After Primary Percutaneous Coronary Intervention in a Middle-Aged Anabolic Steroid–Abusing Bodybuilder
,
Clinical Case
,
Kazuma Tashiro , Yoshitaka Iso , Miki Tsujiuchi , Hiromoto Sone , Masahiro Sasai , Hiroyoshi Mori , Daisuke Wakatsuki , Makoto Shoji , Tokutada Sato , and Hiroshi Suzuki
J Am Coll Cardiol Case Rep. Dec 23, 2020. Epublished DOI: 10.1016/j.jaccas.2020.09.038
,
Abstract
,
A 54-year-old male bodybuilder who was abusing anabolic steroids developed an acute ST-segment elevation myocardial infarction after strenuous strength training. Despite optimal use of dual antiplatelet therapy, on day 4 after primary coronary stenting, the patient suffered another acute coronary event due to subacute thrombosis, potentially pre-disposed by anabolic steroid use. (Level of Difficulty: Intermediate.)
,
History of Presentation
,
A 54-year-old male bodybuilder presented to the emergency department with an episode of acute severe substernal chest pain accompanied by nausea, which had begun after strenuous strength training at midnight and worsened during showering after training. The pain started 3 h before his arrival to the emergency department. He had no precordial angina before the acute events.
,
Learning Objectives
,
•
- To consider the possibility of abuse of performance-enhancing drugs such as AAS in acute coronary events in athletes or exercise enthusiasts.
•
- To recognize the risk and management of subacute thrombosis after a percutaneous coronary intervention.
•
- To understand the side effects of AAS on the cardiovascular system.
,
Based on the patient’s clinical presentation and the initial electrocardiogram (ECG) findings (Supplemental Figure 1A) on arrival, myocardial infarction (MI) was diagnosed. Coronary angiography on arrival revealed total occlusion at the distal portion of the right coronary artery (Figure 1A). Arterial plaque rupture and thrombus formation at the site were documented by optical coherence tomography (OCT). An everolimus-eluting stent was implanted at the site, with a significant improvement in coronary flow. Optimal stent position was confirmed in a final evaluation by OCT after implantation (Figure 1B). Medical treatment after admission included aspirin 100 mg/day and prasugrel 3.75 mg/day (after a loading dose of 20 mg).
,
RCAG and OCT
,
On day 4 after admission, the patient again presented with chest pain. His systolic blood pressure decreased to 60 mm Hg with a heart rate of 40 beats/min and arterial oxygen saturation of 98%. On physical examination, lung and heart sounds were normal with no peripheral edema.
,
Medical History
,
The patient reported nonmedical use of androgen and anabolic steroids (AAS), oral oxandrolone (20 mg) and methandienone (40 mg) daily. He was training systematically for a world-class bodybuilding competition and had been taking the AAS cyclically with 3 months “on” and 1 month “off” in addition to protein supplements for the last 3 years. He had restarted the “AAS-on” phase 2 months before the admission and took the AAS on the day of the acute event.
,
The patient underwent a private periodic health evaluation 3 months before admission. Dyslipidemia and liver dysfunction were detected by fasting blood tests as follows: low-density lipoprotein cholesterol, 150 mg/dl; high-density lipoprotein cholesterol, 32 mg/dl; triglycerides, 148 mg/dl; aspartate aminotransferase, 105 IU/l; and alanine aminotransferase, 272 IU/l. He was a nonsmoker and a social drinker. There was no history of diabetes, hypertension, cardiovascular diseases, or significant family history.
,
Differential Diagnosis
,
The differential diagnosis of chest pain occurring in a subacute phase after acute MI included cardiac free wall rupture, ventricular septal perforation, coronary spasm, or subacute stent thrombosis.
,
Investigations
,
The ECG performed during the patient’s chest pain showed ST-segment elevation in the inferior leads with complete atrioventricular block (Supplemental Figure 1B). Immediate intravenous infusion of heparin and a temporary pacemaker insertion resolved his symptoms. A repeat ECG revealed a normal sinus rhythm. Emergent coronary angiography and OCT revealed a residual nonoccluding thrombus at the site of stent implantation (Figure 1C). Additional coronary angioplasty was not performed. The absence of stent malposition or coronary dissection by the stent edges was confirmed by using OCT. Blood investigations showed no abnormalities in platelet count or coagulation profile (Table 1). A VerifyNow assay (Instrumentation Laboratory, Bedford, Massachusetts) was also performed to evaluate platelet function on the day of the thrombotic event and indicated the optimal dose of dual antiplatelet therapy.
,
Table 1
,
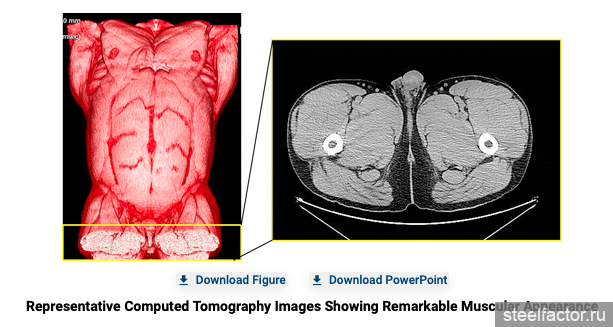
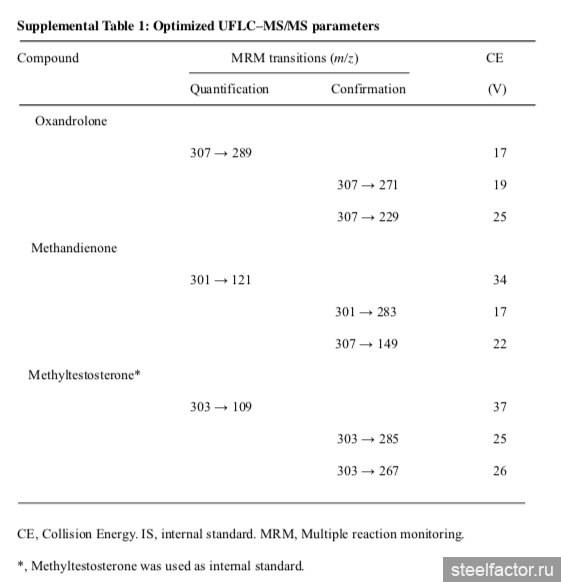
On echocardiogram, concentric left ventricular hypertrophy with a maximum wall thickness of 14 mm was noted. We thus conceived that the thrombotic events might be conferred in part by the AAS abuse. Total and free testosterone concentrations were measured in serum samples on day 7. We found low levels of total and free testosterone (Table 1). However, the patient had no clinical symptoms associated with late-onset hypogonadism. In addition, his weight and body mass index were 111.6 kg and 36.9 kg/m2, respectively, with the remarkable muscular appearance (Figure 2) on admission. Because AAS are synthetic agents, ultra-fast liquid chromatography–tandem mass spectrometry was performed to detect oxandrolone and methandienone in peripheral blood, as previously described (1). For the analyte compounds obtained, the mass spectra were detected in positive-ion electrospray ionization (Supplemental Table 1). Only the presence of the oxandrolone compound was detected in the patient plasma (Figure 3). A quantitative analysis showed 0.28 ng/ml of the oxandrolone concentration.
,
Analysis of Oxandrolone in Human Plasma by UFLC-MS/MS
,
(A) The enhanced product ion spectra obtained from the control human plasma sample spiked with 0.5 ng/ml of oxandrolone (upper) and the patient plasma sample (lower). ( Multiple reaction monitoring chromatograms obtained from the control human plasma sample (upper), the control human plasma spiked with 1.0 ng/ml of oxandrolone (middle), and the patient plasma sample (lower). Red arrows indicate the presence of oxandrolone in the plasma. ESI = electrospray ionization; [M+H]+ = protonated ion; m/z = mass to charge; UFLC-MS/MS = ultra-fast liquid chromatography–tandem mass spectrometry.
Multiple reaction monitoring chromatograms obtained from the control human plasma sample (upper), the control human plasma spiked with 1.0 ng/ml of oxandrolone (middle), and the patient plasma sample (lower). Red arrows indicate the presence of oxandrolone in the plasma. ESI = electrospray ionization; [M+H]+ = protonated ion; m/z = mass to charge; UFLC-MS/MS = ultra-fast liquid chromatography–tandem mass spectrometry.
,
Management
,
Despite optimal use of dual antiplatelet therapy, the patient experienced subacute stent thrombosis. A recent meta-analysis (2) indicated that dual antiplatelet therapy with warfarin or direct oral anticoagulants, including apixaban, could reduce the risk of stent thrombosis. There was no difference in the efficacy between warfarin and direct oral anticoagulants. In the current case, blood examination showed liver dysfunction, which potentially disturbed the warfarin titration. We therefore decided to additionally administer a direct oral anticoagulant (apixaban 10 mg/d). Anticoagulation therapy with dual antiplatelet therapy was continued for 2 weeks, after which aspirin was stopped. Early withdrawal of aspirin might expose the patient to an increased risk of new stent thrombosis. However, the patient discontinued taking the AAS, which might lower the risk. Also, current guidelines in our country (3) propose that aspirin should be stopped within 14 days after percutaneous coronary intervention to decrease bleeding, although there is no evidence regarding the timing of aspirin discontinuation.
,
Discussion
,
AAS are synthetic testosterone analogues and known as sports performance–enhancing drugs. High-dose or multiple AAS abuse has been associated with serious side effects, including cardiovascular adverse events such as dyslipidemia, hypertension, and cardiac hypertrophy (4). Although acute MI is possibly the most devastating complication, limited case reports have reported its association with abuse of AAS (5). This report is the first to describe subacute thrombosis after coronary stenting following an acute MI in a patient with abuse of AAS.
,
Subacute thrombosis is a rare event in the current drug-eluting stent era. In this context, subacute thrombosis occurred in the patient without an underlying thrombotic disorder despite the current recommended use of antiplatelet therapy after coronary stenting without any procedural failure. Its specific cause was not fully clear. However, abuse of AAS likely predisposed him to this event. Thrombogenicity induced by AAS has been suggested by the experimental data. Animals pretreated with AAS exhibited greater clot size and enhanced platelet aggregation (5). Long-term abuse of AAS can decrease testes function, which leads to low levels of intrinsic testosterone, as seen in the present case. In addition, a small but sustained presence of the oxandrolone compound was detected in the patient’s peripheral blood after admission. Methandienone was not found, probably due to a shorter half-life than that of oxandrolone. We thus surmise that acute MI and subacute thrombosis were caused at least in part by the thrombotic activity enhanced by AAS.
,
Prevention of subacute stent thrombosis remains to be explored. The approved dose of prasugrel (3.75 mg/d) in Japan is much lower than that in other countries (10 mg/d). It is not clear whether this dosage is appropriate for overweight Japanese patients. Also, optimal antithrombotic therapy to prevent the recurrence of stent thrombosis needs to be determined. The role of a VerifyNow assay seems to be limited in predicting and identifying the cause of stent thrombosis because stent thrombosis is conferred by several factors such as local coagulation activity. Further studies will be needed to address these issues.
,
Follow-Up
,
The patient was referred to a comprehensive cardiac rehabilitation program in the rehabilitation hospital for secondary prevention and advised to discontinue use of AAS and vigorous exercise training.
,
Conclusions
,
This report presents a unique case of exercise-related acute MI followed by subacute thrombosis, potentially predisposed by abuse of AAS.
In senior athletes and people who exercise vigorously, coronary artery disease is the most common cause of sports-related sudden cardiac death (6). Performance-enhancing drugs such as AAS could potentially enhance cardiovascular risks. Thus, to prevent sudden cardiac events, clinicians should warn athletes about cardiovascular toxicity induced by AAS.
,
Author Relationship With Industry
,
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
,
Abbreviations and Acronyms
,
ECG
electrocardiogram
MI
myocardial infarction
OCT
optical coherence tomography
,
Footnotes
,
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the JACC: Case Reports author instructions page.

0 пользователей, 1 гостей, 0 скрытых


 Наверх
Наверх




 10000000_3566915003428352_3485176809399441447_n.mp4
10000000_3566915003428352_3485176809399441447_n.mp4